




individuals with allergic contact dermatitis could have chronic or relapsing dermatitis, particularly if the material(s) to which they're allergic is not recognized or in the event that they practice inappropriate skin care. The longer an individual has severe dermatitis, the longer, it's believed, that the dermatitis will take to unravel once the cause is recognized.
crucial update: Allergic contact dermatitis as a result of non-latex rubber gloves
In a learn about of surgical operation personnel in Sweden with occupational allergic contact dermatitis, Pontén et al discovered proof that the situation used to be caused by 1,three-diphenylguanidine (1,3-DPG) in non-latex rubber gloves.[1] the usage of patch assessments, the investigators discovered that 12 of 16 patients reacted to 1,three-DPG. The 1,three-DPG used to be present in the gloves worn via the patients within the learn about, with the next concentration on the inside of the gloves than on the skin. In 7 of eight sufferers, contact allergic reaction to cetylpyridinium chloride was also discovered[1]
signs and symptoms
Acute allergic contact dermatitis is characterised via pruritic papules and vesicles on an erythematous base. Lichenified pruritic plaques may indicate a continual form of the situation.
individuals with allergic contact dermatitis most often boost the situation inside a couple of days of publicity, in areas that have been uncovered immediately to the allergen. certain allergens (eg, neomycin), then again, penetrate intact pores and skin poorly; in such circumstances, the onset of dermatitis could also be delayed for as much as every week following exposure.
individuals could boost well-liked dermatitis from topical medicines utilized to leg ulcers or from go-reacting systemic medicines administered intravenously.
Intraoral metallic contact hypersensitivity could end in mucositis that mimics lichen planus, which has an association with intraoral squamous cell carcinoma.
See clinical Presentation for extra element.
prognosis
Diagnostic research for allergic contact dermatitis embody the next:
Potassium hydroxide guidance and/or fungal tradition: To exclude tinea; these checks are ceaselessly indicated for dermatitis of the hands and feet Patch checking out: To identify external chemical substances to which the particular person is allergicRepeat open software test (ROAT): To determine whether a response is very important in folks that enhance weak or 1+ sure reactions to a chemical Dimethylgloxime take a look at: To determine whether a metal object comprises enough nickel to provoke allergic dermatitisSkin biopsy: could lend a hand to exclude different disorders, specifically tinea, psoriasis, and cutaneous lymphoma
See Workup for more element.
administration
The definitive treatment for allergic contact dermatitis is the identification and elimination of any attainable causal marketers; in any other case, the patient is at elevated chance for persistent or recurrent dermatitis. remedies also embrace the next:
Corticosteroids: Topical corticosteroids are the mainstay of treatment, even though acute, extreme allergic contact dermatitis, corresponding to from poison ivy, regularly must be treated with a 2-week direction of systemic corticosteroids Topical immunomodulators (TIMs): authorized for atopic dermatitis, but they're additionally prescribed for circumstances of allergic contact dermatitis once they offer security advantages over topical corticosteroids Phototherapy: Administered to individuals with persistent allergic contact dermatitis that's not managed neatly by using topical corticosteroids; these sufferers may just make the most of remedy with a combination of psoralen (a photosensitizer) and ultraviolet-A (PUVA) Immunosuppressive marketers: power immunosuppressive retailers are, in rare circumstances, used to treat recalcitrant circumstances of severe, power, standard allergic contact dermatitis or severe hand dermatitis that forestalls a affected person from working or performing day by day actions Disulfiram: occasionally, a person who is highly allergic to nickel and has extreme vesicular hand dermatitis will benefit from remedy with disulfiram (Antabuse); the drug has a chelating impact
See treatment and drugs for more element.
image library
 chronic stasis dermatitis with allergic contact dermatitis to quaternium-15, a preservative in moisturizer. Allergic contact dermatitis produces areas of erythema in areas of atrophie blanche and varicose veins. NextBackground
chronic stasis dermatitis with allergic contact dermatitis to quaternium-15, a preservative in moisturizer. Allergic contact dermatitis produces areas of erythema in areas of atrophie blanche and varicose veins. NextBackgroundAllergic contact dermatitis (ACD) is a delayed type of caused sensitivity (allergic reaction) as a result of cutaneous contact with a selected allergen to which the affected person has developed a specific sensitivity. This allergic reaction motives inflammation of the pores and skin manifested by means of varying levels of erythema, edema, and vesiculation.
The time period contact dermatitis once in a while is used incorrectly as a synonym for allergic contact dermatitis. Contact dermatitis is inflammation of the skin precipitated by way of chemicals that right away injury the skin (see Irritant Contact Dermatitis) and by way of specific sensitivity in the case of allergic contact dermatitis.
Jadassohn first described allergic contact dermatitis in 1895. He developed the patch take a look at to establish the chemical substances to which the patient was once allergic. Sulzberger popularized patch trying out in the us in the Nineteen Thirties. The Finn chamber approach for patch trying out used to be designed within the 1970s; these chambers consist of small steel cups, typically attached to strips of tape, stuffed with allergens dispersed in either petrolatum or water. the skinny-layer fast use epicutaneous (proper) check for patch trying out turned into to be had in the united states within the Nineteen Nineties.
The importance of specific materials as reasons of allergic contact dermatitis varies with the incidence of that substance in the atmosphere. Mercury compounds as soon as have been significant causes of allergic contact dermatitis but rarely are used as topical drugs and, at the moment, are distinct as a result in of allergic contact dermatitis. Ethylenediamine, which used to be existing in the unique Mycolog cream, declined as a main result in of allergic contact dermatitis once Mycolog cream was reformulated to not contain this allergen.
a detailed history, both ahead of and after patch trying out, is a very powerful in evaluating people with allergic contact dermatitis. before patch testing, the history identifies doable causes of allergic contact dermatitis and the materials to which people are exposed that should be incorporated in patch testing. After patch checking out, the historical past determines the clinical significance of the findings. (See clinical.)
Topical corticosteroids are the mainstay of therapy, whereas a variety of symptomatic treatments can present brief-term relief of pruritus. alternatively, the definitive therapy of allergic contact dermatitis is the identification and removing of any doable causal retailers; in any other case, the patient is at increased risk for persistent or recurrent dermatitis. (See treatment.)
Go to Irritant Contact Dermatitis, Pediatric Contact Dermatitis, and Protein Contact Dermatitis for full knowledge on these issues.
PreviousNextPathophysiology
roughly 3000 chemical substances are smartly documented as specific causes of allergic contact dermatitis.
Compounds need to be less than 500 d for environment friendly penetration throughout the stratum corneum barrier, which is the water-impermeable outer layer of the skin. Small organic molecules that are chemically reactive (chemical sensitizers) bind with self-proteins to generate immunogenic neoantigens via a process termed haptenization. even supposing haptens can penetrate via intact pores and skin, sufferers with certain illness states that impair barrier perform (eg, leg ulcers, perianal dermatitis) have an increased chance of sensitization to topically utilized medicines and their vehicle elements.
Many sufferers with atopic dermatitis or allergic contact dermatitis to nickel harbor a faulty form of the filaggrin gene.[2] Filaggrin helps combination cytoskeletal proteins that form the cornified cell envelope. In its absence, the barrier is flawed.
Prehaptens are chemical substances that aren't activated through host proteins, but as an alternative require chemical transformation via oxidative derivatization by ambient or air oxidation to form hydroperoxide. Examples embody sure heady scent materials and dyes utilized in hair coloring, akin to para-phenylenediamine.
Haptens activate Toll-like receptors (TLRs) and prompt innate immunity. The importance of hapten-mediated activation of innate immunity is highlighted via the clinical remark that the irritancy of chemical substances (ie, the ability of those chemical substances to cause grossly visible skin irritation upon primary publicity) correlates with their capacity to act as contact sensitizers and to induce acute contact dermatitis.
Haptens or haptenated self-proteins are recognized through innate immune mechanisms in the skin, and this results in the elaboration of plenty of proinflammatory mediators, including interleukin (IL)–1β. because of this, pores and skin-resident dendritic cells (DCs) develop into activated. There are a couple of populations of DCs. Langerhans cells are the one DC subtype within the dermis. like every pores and skin-resident DCs, Langerhans cells efficiently accumulate antigen in the periphery and migrate to regional lymph nodes the place they existing antigen to naïve and reminiscence T cells. These DCs, which will have been directly haptenated or can have obtained haptenated proteins from their environment, migrate to skin-draining lymph nodes the place they existing peptides from haptenated proteins to set off memory and naïve T cells.
within the last step, hapten-caused irritation recruits activated effector T cells back to the preliminary website online of antigen come across in the skin. The effector T cells unencumber proinflammatory cytokines, equivalent to interferon-γ, and promote the killing of haptenated cells, resulting in the construction of the basic inflammatory rash considered in allergic contact dermatitis.
Keratinocytes are a very powerful for the advance of allergic contact dermatitis. They constitute the overwhelming majority of cells within the epidermis and form the anatomic barrier of the skin. Keratinocytes specific most TLRs, and this allows them to answer TLR4-triggering haptens, equivalent to nickel. Keratinocytes are additionally a source of IL-10, an immunosuppressive cytokine that limits the extent of contact hypersensitivity
The initial sensitization generally takes 10-14 days from initial publicity to a strong contact allergen corresponding to poison ivy. Some individuals enhance explicit sensitivity to allergens following years of chronic low-grade exposure; for example, sensitivity to chromate in cement can ultimately develop in people with power irritant contact dermatitis attributable to the alkaline nature of cement. as soon as an individual is sensitized to a chemical, allergic contact dermatitis develops within hours to a number of days of publicity.
CD4+ CCR10+ reminiscence T cells persist within the dermis after scientific decision of allergic contact dermatitis.
PreviousNextEtiology
roughly 25 chemicals look like accountable for as many as one 1/2 of all cases of allergic contact dermatitis. These embody nickel, preservatives, dyes, and fragrances.
Poison ivy
Poison ivy (Toxicodendron radicans) is the basic example of acute allergic contact dermatitis in North the united states. Allergic contact dermatitis from poison ivy is characterized by means of linear streaks of acute dermatitis that improve where plant parts had been in direct contact with the pores and skin.
Nickel
Nickel is the leading result in of allergic contact dermatitis in the world. The incidence of nickel allergic contact dermatitis in North america is rising; in distinction, new laws in Europe have resulted in a reducing incidence of nickel hypersensitivity in young and heart-aged ladies.[3, 4]
Allergic contact dermatitis to nickel generally is manifested via dermatitis on the web sites the place rings or necklaces (see the image beneath) containing nickel are worn or the place metallic objects (together with the keypads of some cell phones[5] ) containing nickel are in touch with the pores and skin.
Nickel is also regarded as a conceivable occupational allergen. employees in whom nickel is also an occupational allergen primarily include hairdressers, retail clerks, caterers, domestic cleaners, and metalworkers. people allergic to nickel every so often could advance vesicles on the sides of the fingers (dyshidrotic hand eczema or pompholyx) from nickel within the weight-reduction plan.
 Allergic contact dermatitis to nickel in a necklace. Rubber gloves
Allergic contact dermatitis to nickel in a necklace. Rubber glovesallergic reaction to 1 or more chemicals in rubber gloves is recommended in any individual with continual hand dermatitis who wears them, except patch checking out demonstrates otherwise. Allergic contact dermatitis to chemical compounds in rubber gloves typically happens maximally on the dorsal elements of the hand. frequently, a cutoff of dermatitis happens on the forearms where skin is no longer in contact with the gloves. individuals allergic to chemical compounds in rubber gloves could improve dermatitis from different exposures to the chemical compounds (eg, under elastic waistbands).
Hair dye and transient tattoos
p-Phenylenediamine (PPD) is a typical section of and sensitizer in everlasting hair dye products and brief henna tattoos[6] ; publicity in to it in hair dye products could result in acute dermatitis with extreme facial edema. severe local reactions from PPD may just occur in black henna tattoos in adults and children. Epidemiologic information point out that the median occurrence of certain patch check reactions to PPD among dermatitis patients is four.three% (growing) in Asia, four% (plateau) in Europe, and 6.2% (decreasing) in North the us.[7]
Textiles
people allergic to dyes and permanent press and wash-and-wear chemicals delivered to textiles typically advance dermatitis on the trunk, which occurs maximally on the lateral sides of the trunk but spares the vault of the axillae. main lesions could also be small follicular papules or may be in depth plaques.
individuals in whom this allergic contact dermatitis is suspected must be examined with a collection of fabric chemicals, particularly if movements patch testing reveals no allergic reaction to formaldehyde. New garb is perhaps to provoke allergic contact dermatitis, for the reason that most allergens decrease in concentration in apparel following repeated washings.
Preservatives
Preservative chemical compounds introduced to cosmetics, moisturizers, and topical medications are main reasons of allergic contact dermatitis (see the picture below). the chance of allergic contact dermatitis appears to be best possible to quaternium-15, followed by way of allergic contact dermatitis to isothiazolinones. Kathon CG is methylchloroisothiazolinone in combination with methylisothiazolinone.
Methylisothiazolinone is now used as an individual preservative and could also be a significant allergen.[8]
even though parabens are among the many most generally used preservatives, they don't seem to be a established cause of allergic contact dermatitis.
 extreme allergic contact dermatitis as a result of preservatives in sunscreen. Patch testing was terrible to the active ingredients within the sunscreen.
extreme allergic contact dermatitis as a result of preservatives in sunscreen. Patch testing was terrible to the active ingredients within the sunscreen.Schnuch et al estimated that preservatives present in leave-on topical products varied over 2 orders of magnitude in relative sensitization risk.[9]
Formaldehyde is an incredible result in of allergic contact dermatitis (see the picture beneath). sure preservative chemicals widely utilized in shampoos, lotions, other moisturizers, and cosmetics are termed formaldehyde releasers (ie, quaternium-15 [Dowicil 200], imidazolidinyl urea [Germall 115], and isothiazolinones[9] ).
 Onycholysis creating from allergic contact dermatitis to formaldehyde used to harden nails. Fragrances
Onycholysis creating from allergic contact dermatitis to formaldehyde used to harden nails. Fragrancespeople may just increase allergy to fragrances. Fragrances are discovered not handiest in perfumes, colognes, aftershaves, deodorants, and soaps, but additionally in a lot of different products, ceaselessly as a masks to camouflage an unpleasant smell. Unscented merchandise could contain fragrance chemical substances used as a portion of the product and no longer labeled as scent.
folks allergic to fragrances should use scent-free products. sadly, the exact chemical compounds answerable for a scent in a product aren't labeled. 4 thousand totally different scent molecules are to be had to formulate perfumes. The fragrance business shouldn't be required to free up the names of elements used to compose a fragrance in the U.S., even when people boost allergic contact dermatitis to fragrances found in topical medications.
Deodorants is also the most common cause of allergic contact dermatitis to fragrances as a result of they are utilized to occlude pores and skin that is frequently abraded by way of shaving in girls.
massage and bodily therapists and geriatric nurses are at greater risk of occupational allergic contact dermatitis to fragrances.
Corticosteroids
within the final decade, it has develop into clear that some individuals with persistent dermatitis strengthen hypersensitive reaction to topical corticosteroids. Most affected people may also be treated with some topical corticosteroids, however an individual can also be allergic to all topical and systemic corticosteroids. Budesonide and tixocortol pivalate are useful patch take a look at corticosteroids for making a choice on individuals allergic to topical corticosteroids.
Neomycin
the danger of hypersensitive reaction to neomycin is said instantly to the extent of its use in a inhabitants. the risk of allergy to neomycin is way larger when it is used to treat continual stasis dermatitis and venous ulcers than when it is used as a topical antibiotic on cuts and abrasions in children. think that people allergic to neomycin are allergic to chemically related aminoglycoside antibiotics (eg, gentamicin, tobramycin).[10] avoid these medicine each topically and systemically in folks allergic to neomycin.
Benzocaine
steer clear of topical use of benzocaine. Benzocaine is integrated in most same old patch check trays. people allergic to benzocaine may safely use or be injected with lidocaine (Xylocaine), which does not move-react with benzocaine.
a lot of people complain of adversarial reactions to sunscreens, but many of those people are no longer allergic to the sunscreen supplies. They is also allergic to preservatives in these products or can have nonspecific cutaneous inflammation from these products.
Photoallergy
now and again, folks strengthen photoallergic contact dermatitis. Allergic contact dermatitis is also accentuated by ultraviolet (UV) gentle, or sufferers may just improve an allergy handiest when a chemical is present on the pores and skin and when the skin is exposed sufficiently to ultraviolet light A (UV-A; 320-four hundred nm).
PreviousNextEpidemiologyUnited States data
The national well being and nutrition Examination Survey (NHANES) estimated the incidence of contact dermatitis to be 13.6 cases per a thousand inhabitants, the usage of bodily examinations by means of dermatologists of a specific pattern of sufferers. NHANES underreported the prevalence when put next with the physical examination findings.
The nationwide Ambulatory hospital therapy Survey performed in 1995 estimated eight.4 million outpatient visits to American physicians for contact dermatitis. This was the second most common dermatologic diagnosis. Of place of job visits to dermatologists, 9% are for dermatitis. At a student health middle dermatology health facility, 3.1% of sufferers introduced for allergic contact dermatitis, and a couple of.three% introduced for irritant contact dermatitis.
The authentic check site can present accurate normal knowledge on widespread allergens. The Contact Allergen administration program is equipped as a service to the American Contact Dermatitis Society (ACDS) contributors and is especially precious for allergens present in topical skin care products. The Contact Allergen substitute Database (CARD) incorporates more than 8100 known ingredients cataloged in additional than 5500 commercial skincare merchandise and is available as a Smartphone software.
international records
A Swedish study discovered that incidence of allergic contact dermatitis of the fingers used to be 2.7 circumstances per a thousand population. A Dutch learn about discovered that occurrence of allergic contact dermatitis of the arms was 12 instances per one thousand inhabitants.
Race, sex, and age-related demographics
No racial predilection exists for allergic contact dermatitis. Allergic contact dermatitis is extra fashionable in ladies than in males. This predominantly is as a result allergic reaction to nickel, which is rather more well-liked in women than in men in most nations.
Allergic contact dermatitis may just happen in neonates. In elderly individuals, the improvement of allergic contact dermatitis could also be delayed rather, but the dermatitis may be more continual as soon as developed. Contact hypersensitivity to topical medicaments is extra in style in individuals older than 70 years.[11]
PreviousNextPrognosis
individuals with allergic contact dermatitis may have power or relapsing dermatitis, in particular if the material(s) to which they are allergic shouldn't be recognized or in the event that they proceed to follow skin care that's not appropriate (ie, they proceed to make use of harsh chemical compounds to wash their pores and skin, they do not observe creams with ceramides or bland emollients to protect their skin).
The longer a person has severe dermatitis, the longer it's believed it's going to take the dermatitis to unravel as soon as the lead to is identified.
Some folks have power dermatitis following allergic contact dermatitis, which seems to be authentic especially in folks allergic to chrome.
a selected problem is neurodermatitis (lichen simplex chronicus), wherein individuals many times rub or scratch a neighborhood initially affected by allergic contact dermatitis.
Mortality
death from allergic contact dermatitis is unusual in the united states. Allergic contact dermatitis to the weed wild feverfew brought about deaths in India when the seeds contaminated wheat shipments to India. This plant then become in style and a first-rate lead to of severe airborne allergic contact dermatitis.
PreviousNextPatient schooling
patients have one of the best prognosis when they are able to understand that the materials to which they are allergic and the best way to steer clear of further exposures. present sufferers with as so much knowledge as possible regarding the chemical to which they're allergic, including all recognized names of the chemical. internet sites, Smartphone applications, same old textbooks, and the real test kit incorporate normal details about the chemicals.
vulnerable people want to learn the record of ingredients earlier than applying cosmetic merchandise to their pores and skin, on account that preservative chemical compounds are used extensively in client, medical, and place of work merchandise. the same chemical can have totally different names when used for consumer or industrial functions.
provide pamphlets with coloration footage of poison ivy to individuals allergic to the plant. The American Academy of Dermatology also has pamphlets on allergic contact dermatitis and hand eczema.
For affected person schooling knowledge, see the pores and skin, Hair, and Nails center, as well as Contact Dermatitis.
PreviousProceed to medical Presentation , Allergic Contact Dermatitis
 Stevens-Johnson syndrome. NextBackground
Stevens-Johnson syndrome. NextBackground Morbilliform drug eruption.
Morbilliform drug eruption. Urticaria. kind II is cytotoxic reactions, which result in hemolysis and purpura (see the picture beneath).
Urticaria. kind II is cytotoxic reactions, which result in hemolysis and purpura (see the picture beneath). Oral ulcerations in a affected person receiving cytotoxic remedy. sort III is immune advanced reactions, which lead to vasculitis, serum sickness, and urticaria.sort IV is delayed-kind reactions with cell-mediated hypersensitivity, which result in contact dermatitis, exanthematous reactions, and photoallergic reactions.
Oral ulcerations in a affected person receiving cytotoxic remedy. sort III is immune advanced reactions, which lead to vasculitis, serum sickness, and urticaria.sort IV is delayed-kind reactions with cell-mediated hypersensitivity, which result in contact dermatitis, exanthematous reactions, and photoallergic reactions. Phototoxic reaction after use of a tanning sales space. be aware sharp cutoff the place garb blocked publicity. PreviousNextFrequencyUnited States
Phototoxic reaction after use of a tanning sales space. be aware sharp cutoff the place garb blocked publicity. PreviousNextFrequencyUnited States Amiodarone pigmentation.
Amiodarone pigmentation. This patient has a splenic abscess because of pneumococcal bacteremia. note that the vastly enlarged spleen is quickly visible, with minimal retraction in the left upper quadrant.
This patient has a splenic abscess because of pneumococcal bacteremia. note that the vastly enlarged spleen is quickly visible, with minimal retraction in the left upper quadrant. 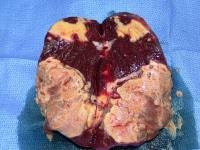 Resected specimen from the affected person in the previous image. notice the discrete abscesses adjacent to customary parenchyma. Inflammatory splenomegaly
Resected specimen from the affected person in the previous image. notice the discrete abscesses adjacent to customary parenchyma. Inflammatory splenomegaly