






Cerebrospinal fluid (CSF) contains a mixture of water, electrolytes (Na+, k+, Mg2+, Ca2+, Cl-, and HCO3-), glucose (60-eighty% of blood glucose), amino acids, and more than a few proteins (22-38 mg/dL). CSF is colorless, clear, and typically devoid of cells equivalent to polymorphonuclear cells and mononuclear cells (
the principle web site of CSF production is the choroid plexus, which is liable for 50-eighty% of its daily production. different web sites of manufacturing embrace the ependymal surface layer (as much as 30%) and capillary ultrafiltration (as much as 20%). CSF represents the top made from the ultrafiltration of plasma across epithelial cells within the choroid plexus lining the ventricles of the brain. A basal layer Na+/ok+ ATPase is chargeable for actively transporting Na+ into epithelial cells, after which water follows across this gradient. Carbonic anhydrase catalyzes the formation of bicarbonate within the epithelial cell. any other Na+/okay+ ATPase lining the ventricular facet of the epithelium extrudes Na+ into the ventricle, with water following throughout this ionic gradient. The ensuing fluid is termed cerebrospinal fluid.
CSF is produced at a fee of roughly 20 mL/h for a total of approximately 500 mL daily. At any given time, approximately ninety-one hundred fifty mL of CSF is circulating all through the CNS. CSF produced at the choroid plexus typically circulates from the lateral ventricles to the third ventricle by way of the aqueduct of Sylvius. From the 0.33 ventricle, the fluid circulates into the forth ventricle and out into the subarachnoid house via the foramina of Magendie and Luschka. After circulating in the course of the subarachnoid space, CSF is reabsorbed by way of the arachnoid villi.
Circulation of CSF is maintained by means of the hydrostatic variations between its fee of production and its charge of absorption. standard CSF force is roughly 10-15 mm Hg, and accelerated drive constitutes an intracranial power (ICP) better than 20 mm Hg.
CSF rhinorrhea is a uncommon however doubtlessly devastating condition that may result in vital morbidity and mortality for the patient. Disruption of the limitations between the sinonasal cavity and the anterior and center cranial fossae is the underlying issue resulting in the discharge of CSF into the nasal cavity. The resulting verbal exchange with the CNS may end up in a mess of infectious problems that impart significant morbidity and probably disastrous long-time period deficits for the patient.
this article discusses present ideas in the etiology, diagnosis, and therapy of CSF rhinorrhea, in addition to lengthy-time period management of sufferers following a hit treatment.
See the picture beneath.
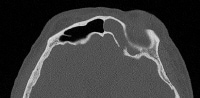 An axial CT of a patient with a spontaneous CSF leak finds a defect within the posterior desk of the left frontal sinus. NextHistory Of The procedure
An axial CT of a patient with a spontaneous CSF leak finds a defect within the posterior desk of the left frontal sinus. NextHistory Of The procedureFrom the primary intracranial restore within the 1900s to using endoscopes and picture-steerage methods, the administration of cerebrospinal fluid (CSF) rhinorrhea has greatly advanced. Dandy is credited with the primary surgical restore of a CSF leak by way of a frontal craniotomy approach in 1926. quite a lot of other authors, together with Dohlman (1948), Hirsch (1952), and Hallberg (1964), therefore said a success restore of CSF rhinorrhea thru totally different external processes. In 1981, Wigand mentioned on the usage of the endoscope to assist with the restore of a skull base defect. considering then, endoscopic restore has change into the most popular method of addressing CSF rhinorrhea, given the excessive success charge of ninety-95% and the diminished morbidity associated with this way.
PreviousNextProblem
The underlying defect chargeable for cerebrospinal fluid (CSF) leaks, whatever the etiology, is the same: disruption within the arachnoid and dura mater coupled with an osseous defect and a CSF drive gradient that is constantly or intermittently greater than the tensile energy of the disrupted tissue.
PreviousNextEpidemiologyFrequency
The frequency of cerebrospinal fluid (CSF) rhinorrhea relies on the underlying etiology. Please refer to Etiology for further important points.
PreviousNextEtiology
Cerebrospinal fluid (CSF) leaks are normally classified as worrying, iatrogenic, and spontaneous/idiopathic. worrying reasons embrace both blunt and penetrating facial injuries. Iatrogenic causes include neurosurgical and otolaryngologic techniques to neoplastic illness, in addition to purposeful endoscopic sinus surgical procedure (FESS). Most spontaneous, or major, reasons of CSF rhinorrhea are now notion in fact to be secondary to elevations in intracranial pressure (ICP) that might be seen in patients with idiopathic intracranial hypertension (IIH). Congenital skull base defects and sure tumors can also result in CSF rhinorrhea.
traumatic CSF rhinorrhea
Penetrating and closed-head trauma are answerable for ninety% of all circumstances of CSF leaks. CSF rhinorrhea following a annoying damage is classified as quick (inside 48 hours) or delayed. nearly all of sufferers with a CSF leak because of unintended trauma (eg, motor car accident) current instantly. lots of the sufferers (95%) with a delayed CSF leak existing inside 3 months after the damage.
Iatrogenic CSF rhinorrhea
unlike worrying leaks, only 50% of sufferers with iatrogenic CSF leaks current within the first week after the insult. usually, the affected person will have been discharged when the leak items itself. hence, educating the patient relating to the standard signs related to a CSF leak comparable to salty or metal taste is of paramount significance.
Any surgical manipulation close to the skull base can lead to an iatrogenic CSF leak. cranium base accidents can differ from easy cracks in the bony architecture to very large (>1 cm) defects with disruption of the dura and probably brain parenchyma.
Otolaryngology approaches, including FESS and septoplasty, can lead to a cranium base defect and CSF rhinorrhea. certain neurosurgical processes akin to craniotomy and transsphenoidal pituitary resections are most repeatedly associated with an elevated chance of CSF rhinorrhea.
In sufferers undergoing endoscopic sinus surgery, the website online of damage is most frequently the lateral lamella of the cribriform plate, where the bone of the anterior cranium base is thinnest. different in style areas embody the posterior fovea ethmoidalis and the posterior facet of the frontal recess.
Tumor-related CSF rhinorrhea
the growth of benign tumors does now not regularly end in CSF rhinorrhea. then again, in the community aggressive lesions akin to inverted papilloma and malignant neoplasms can erode the bone of the anterior cranial fossa. The enzymatic breakdown or destruction of the bony architecture leads to inflammation and attainable violation of the dura. although the tumor itself does now not result in CSF rhinorrhea, the resection in most cases ends up in instant leakage. therefore, the surgical staff will have to be ready to restore the ensuing CSF leak at the time of the resection, both transcranially or endoscopically.
Congenital CSF rhinorrhea
Defects within the closure of the anterior neuropore can lead to the herniation of principal anxious tissue through anterior cranial fossa. These are sometimes related to CSF rhinorrhea. The embryologic defect is normally a patent fonticulus frontalis or foramen cecum. Meningoencephaloceles usually current in childhood as an intranasal/extranasal mass that transilluminates and expands with crying (Furstenberg signal). A high index of suspicion will have to be maintained with all pediatric intranasal plenty, in particular these occurring at the midline. A biopsy should by no means be obtained unless a complete imaging workup has been conducted.
Spontaneous CSF rhinorrhea
Spontaneous CSF rhinorrhea occurs in sufferers with out antecedent motives. This terminology appears to indicate that spontaneous CSF leaks are idiopathic in nature; then again, contemporary proof has led us to comprehend that spontaneous CSF rhinorrhea may in fact be secondary to an intracranial process, particularly elevated intracranial pressure (ICP). There are several causes of accelerated ICP; then again, the proposed mechanism underlying spontaneous CSF rhinorrhea is idiopathic intracranial hypertension (IIH). Obstructive sleep apnea (OSA) has also been linked to accelerated ICP.
regardless of the multifactorial causes of extended ICP, once this drawback ensues, the power exerted on areas of the anterior skull base such as the lateral lamella of the cribriform or lateral recess of the sphenoid sinus ends up in bone reworking and thinning. in some way, a defect is formed. At this point, the dura herniates through the defect (meningocele). If the defect is big, brain parenchyma might also herniate in the course of the defect (encephalocele).
PreviousNextPathophysiology
speedy hectic leaks outcome from a bony defect or fracture at the side of a dural tear. A that you can think of cause of a delayed worrying leak is a previously intact dural layer that has slowly herniated thru a bony defect, at last tearing and allowing the cerebrospinal fluid (CSF) to leak. in step with some other theory, the tear and bony defect are existing from the time of the original injury, however the leak occurs best after the masking hematoma dissolves.
Spontaneous CSF rhinorrhea on a regular basis manifests in maturity, coinciding with a developmental rise in CSF power with maturity. The dura of the anterior cranial base is subject to huge adaptations in CSF power as a result of a couple of elements, together with normal arterial and respiratory fluctuations. different stresses include Valsalva-like maneuvers throughout nose blowing or straining. it will result in dural tears in areas of abnormalities of the bony floor.
increased intracranial power isn't all the time present within the case of spontaneous CSF rhinorrhea. different proposed mechanisms for nontraumatic CSF leaks include focal atrophy, rupture of arachnoid projections that accompany the fibers of the olfactory nerve, and persistence of an embryonic olfactory lumen.
Iatrogenic CSF rhinorrhea results from surgical disruption of the cranium base and dura as in the past mentioned.
PreviousNextPresentationHistory
a thorough history is step one towards accurate diagnosis. the typical historical past of a cerebropsinal fluid (CSF) leak is that of clear, watery discharge, usually unilateral. analysis is made more easily in patients with latest trauma or surgical treatment than in others. Delayed fistulas are troublesome to diagnose and might happen years after the trauma or operation. These instances often result in a misdiagnosis of allergic and vasomotor rhinitis. occasionally, the patient has a history of headache relieved by using drainage of CSF. Drainage is also intermittent as the fluid accumulates in one of the vital paranasal sinuses and drains externally with changes in head position (ie, reservoir sign).
A history of headache and visible disturbances suggests elevated intracranial force. every so often, associated symptoms might actually help in localizing the leak. for example, anosmia (existing in 60% of individuals with publish-hectic rhinorrhea), signifies an harm within the olfactory house and anterior fossa, especially when it's unilateral. Optic nerve deficits counsel a lesion in the area of tuberculum sellae, sphenoid sinus, or posterior ethmoid cells. patients with recurrent meningitis, especially pneumococcal meningitis, must be evaluated for a defect that exposes the intracranial house to the upper airway, regardless of the presence or absence of CSF rhinorrhea.
physical examination
bodily examination should embody complete rhinologic (together with endoscopic), otologic, head and neck, and neurologic reviews. Endoscopy could expose an encephalocele or meningocele. Drainage of CSF in some cases may often be elicited on endoscopy via having the patient operate a Valsalva maneuver or by way of compressing both jugular veins (Queckenstedt-Stookey test). then again, as a rule bodily examination is unrevealing, particularly in patients with intermittent CSF rhinorrhea.
In patients with head trauma, a combination of blood and CSF could make the prognosis tough. CSF separates from blood when it is positioned on filter paper, and it produces a clinically detectable sign: the ring signal, double-ring signal, or halo signal. alternatively, the presence of a hoop sign will not be exclusive to CSF and can lead to false-positive results.[1] unlike unilateral rhinorrhea, bilateral rhinorrhea provides no clue of the laterality of the defect. however, even in this state of affairs, exceptions can happen. Paradoxical rhinorrhea occurs when midline structures that act as separating boundaries (eg, crista galli, vomer) are dislocated. This dislocation permits CSF to go with the flow to the opposite side and manifest at the contralateral naris. The scientific findings most often associated with CSF rhinorrhea are meningitis (30%) and pneumocephalus (30%).
PreviousNextIndications
except medical or surgical contraindications exist, surgical repair is really useful in all sufferers with spontaneous or iatrogenic cerebropsinal fluid (CSF) rhinorrhea in order to prevent ascending meningitis.
In sufferers with nonsurgical trauma, waiting a length of 5-7 days to allow conservative measures (bed relaxation, stool softeners, and lumbar drainage) to help with secondary closure of the anxious defect is reasonable. however, if CSF rhinorrhea persists past this level, or if a big cranium base defect is observed on the time of harm, surgical restore is warranted.
If an iatrogenic leak is detected intraoperatively, it should be repaired at the time of the original surgery. generally of iatrogenic damage offering in a delayed fashion, surgical restore is important. A lumbar drain placed on the time of restore has now not been proven to decrease recurrence of the CSF leak.
PreviousNextRelevant Anatomy
the commonest anatomic sites of spontaneous cerebrospinal fluid (CSF) leaks are the areas of congenital weak spot of the anterior cranial fossa and areas associated to the kind of surgical operation performed. The lateral lamella of the cribriform plate seems to be interested by roughly 40% of the cases, whereas a defect within the region of the fontal sinus is detected 15% of the time. The sella turcica and sphenoid sinus are taken with 15% of the cases as smartly.
in style websites of injury secondary to endoscopic sinus surgical operation include the lateral lamella of the cribriform plate and the posterior ethmoid roof close to the anterior and medial sphenoid wall. rarely, the leak can originate in the center or posterior cranial fossa and can attain the nasal cavity by the use of the center ear and eustachian tube. These sufferers generally existing with aural fullness due to a serous heart ear effusion.
PreviousNextContraindications
Surgical restore of skull base defects resulting in cerebrospinal fluid (CSF) rhinorrhea is contraindicated in any affected person who shouldn't be medically steady to endure a common anesthetic or comply with postoperative care.
The administration of CSF rhinorrhea relies on the cause, region, and severity of the leak. When trauma is the lead to, the interval between trauma and the onset of the leak is important. The natural historical past of CSF rhinorrhea is highly dependant on the underlying etiology.
demanding leaks stop spontaneously within the majority of cases, consequently a conservative approach is best. The leakage stops within 1 week in 70% of patients, inside 3 months in 20-30%, and inside 6 months in most patients. The leak nearly by no means recurs. the alternative is right for nontraumatic leaks, as only one third stop spontaneously. Intermittent leakage over a number of years is attribute.
PreviousProceed to Workup , CSF Rhinorrhea

No comments:
Post a Comment
Note: Only a member of this blog may post a comment.