






Systemic mastocytosis, frequently termed systemic mast cell illness (SMCD), is a myeloproliferative neoplasm characterized by infiltration of clonally derived mast cells in numerous tissues, including bone marrow, skin, the gastrointestinal tract, the liver, and the spleen.[1, 2, 3, 4, 5] Median survival ranges from 198 months in sufferers with indolent systemic mastocytosis to forty one months in aggressive systemic mastocytosis and a pair of months in mast cell leukemia.
very important update: better figuring out of bone involvement in systemic mastocytosis
Indolent systemic mastocytosis with or without cutaneous manifestations is characterized by means of lowered trabecular bone mass and an increased choice of osteoclasts and osteoblasts. In a retrospective learn about of 300 patients with histologically proven indolent systemic mastocytosis, bone cell numbers in patients with mast cell granulomas have been considerably larger than in those with diffuse mast cell distribution. Severity of bone illness in these patients may be dependent on the amount of mast cells and their distribution inside bone marrow rather than the presence or absence of cutaneous involvement.[6]
indicators and signs
Manifestations of systemic mastocytosis may just embrace the next:
Anemia and coagulopathyAbdominal pain is the most typical GI symptom, adopted, with the aid of diarrhea, nausea, and vomitingSymptoms and indicators of gastroesophageal reflux illness (GERD)Pruritus and flushingAnaphylactoid reaction (eg, to Hymenoptera stings, general anesthetics, intravenous contrast media, other drugs, foods)[7, 8]
Findings on bodily examination could include the following:
indicators of anemia (eg, pallor)Hepatomegaly (27%)Splenomegaly (37%)Lymphadenopathy (21%)Urticaria (forty one%)Osteolysis and pathological fractures (uncommon)
See medical Presentation for more detail.
diagnosis
Findings on blood research may just include the next:
Anemia (forty five% of patients)ThrombocytopeniaLeukocytosisSome patients have eosinophilia, basophilia, thrombocytosis, and monocytosisThe aggregate of anemia, thrombocytopenia, hypoalbuminemia, and extra bone marrow blasts (>5%) portends a poor prognosis[9]
size of serum tryptase could reveal the next:
total serum tryptase levels of 20 ng/mL or greater in a baseline serum sample with a total–to–beta-tryptase ratio greater than 20:1[10] Serum tryptase levels of eleven.5 ng/mL or greater (the reduce-off worth used in more latest research) are discovered in additional than 50% of patients
the next imaging research may be important to establish the extent and stage of the illness:
GI radiography, ultrasonography, and liver-spleen computed tomography scanning in sufferers with belly painSkeletal surveys and bone CT scanning in patients with suspected bone involvement
Diagnostic approaches are as follows:
Bone marrow aspiration and biopsy are essentialGI methods (eg, barium studies, endoscopy) are indicated for sufferers with GI symptomsLiver biopsy can convey mast cell infiltration in patients with hepatomegalySkin biopsy could also be warranted in sufferers with cutaneous manifestations
the foremost diagnostic criterion for systemic mastocytosis is the presence of dense infiltrates of mast cells in bone marrow or other extracutaneous tissues. Mast cells must be viewed in aggregates of 15 or more.
major standards is also absent in early illness. on this scenario, the minor criteria are used to make the pathologic diagnosis. Three of the following four minor criteria are required to make the diagnosis:
atypical mast cell morphology in 25% or extra of the mast cellsExpression of CD2 and/or CD25 in addition to normal mast cell markersSerum/plasma tryptase ranges higher than 20 ng/mLA codon-816 c-equipment mutation in peripheral blood, bone marrow, or concerned tissue
kinds of mastocytosis (World health group standards) are as follows:
Cutaneous mastocytosisIndolent systemic mastocytosis (systemic mast cell disease)Systemic mastocytosis with associated clonal hematologic non–mast cell lineage diseaseAggressive systemic mastocytosisMast cell leukemiaMast cell sarcomaExtracutaneous mastocytoma
See Workup for more element.
administration
treatment for systemic mastocytosis is basically symptomatic; no remedy is curative. therapy modalities include the administration of the following:
Anaphylaxis and associated symptomsPruritus and flushingIntestinal malabsorption
sellers for symptomatic reduction embrace the next:
Epinephrine is utilized in acute anaphylaxisH1 and H2 receptor blockers are used to regulate anaphylactic symptomsCorticosteroids had been used to regulate malabsorption, ascites, and bone pain and to prevent anaphylaxisCromolyn is helpful for reducing bone pain and headaches and for making improvements to pores and skin symptomsPatients with osteopenia that doesn't reply to remedy may just obtain a trial of interferon alfa-2bFirst-technology histamine H1 antagonists (eg, diphenhydramine, hydroxyzine) were used to deal with pruritus and flushingHistamine H2 antagonists and proton pump inhibitors have been used to treat gastric hypersecretion and peptic ulcer diseaseAspirin can be used when H1 and H2 receptor blockers do not stop vascular collapseMast cell stabilizers (eg, ketotifen) had been used to treat pruritus and whealingLeukotriene antagonists (eg, zafirlukast, montelukast) have been usedCromolyn is helpful for reducing bone ache and complications and for making improvements to pores and skin symptomsPsoralen ultraviolet A remedy could present transient aid of pruritus and may lead to fading of pores and skin lesionsAnticholinergics have been used within the treatment of diarrheaDisodium cromolyn has been used within the treatment of stomach cramping and diarrhea
Chemotherapy has no longer been in particular successful within the administration of systemic mastocytosis, however the next regimens have been tried[11] :
Interferon-alfa could also be a good idea, particularly in patients with aggressive systemic mastocytosis2-Chlorodeoxyadenosine (Cladribine)Thalidomide in developed diseaseImatinib mesylate (Gleevec) in patients who would not have mutations of the codon 816 on the c-equipment gene and raise the wild-sort package, or who carry the FIP1L1-PDGFRA rearrangement[12]
See remedy and medicine for more element.
picture library
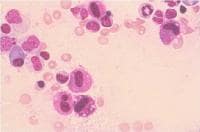 Bone marrow aspirate, Romanowsky stain, excessive-definition magnification. prognosis is mastocytosis, and morphology is strange mast cells. this is a bone marrow smear from a affected person with systemic mastocytosis. a number of mast cells are existing in this photo. These mast cells are larger than customary mast cells and have extra irregularly shaped nuclear outlines and less densely packed mast cell granules. Courtesy of the American Society of Hematology Slide bank. Used with permission. NextBackground
Bone marrow aspirate, Romanowsky stain, excessive-definition magnification. prognosis is mastocytosis, and morphology is strange mast cells. this is a bone marrow smear from a affected person with systemic mastocytosis. a number of mast cells are existing in this photo. These mast cells are larger than customary mast cells and have extra irregularly shaped nuclear outlines and less densely packed mast cell granules. Courtesy of the American Society of Hematology Slide bank. Used with permission. NextBackgroundSystemic mastocytosis, regularly termed systemic mast cell disease (SMCD), is a heterogeneous clonal dysfunction of the mast cell and its precursor cells. it is now categorized as a myeloproliferative neoplasm (MPN) as per the 2008 revision of the WHO classification of myeloid neoplasms.[13] The scientific signs and indicators of systemic mastocytosis (systemic mast cell disease) are due to the buildup of these clonally derived mast cells in several tissues, including bone marrow, skin, the gastrointestinal (GI) tract, the liver, and the spleen.[1, 2, 3, 4, 5]
Systemic mastocytosis (systemic mast cell disease) is characterized by using mast cell infiltration of extracutaneous organs, which is in contrast to cutaneous mast cell problems, which contain best the skin. Ehrlich first described mast cells in 1877 when he found cells that stained metachromatically with aniline dyes.[14] He known as these cells "mast Zellen" since the cells had been distended with granules.
Cutaneous mastocytosis used to be recognized in the late nineteenth century. Sangster first described urticaria pigmentosa, which is likely one of the cutaneous mast cell problems, in 1878. In 1933, Touraine advised that this illness could contain inside organs. In 1949, Ellis first based at post-mortem that cutaneous mastocytosis might also involve inner organs. An post-mortem of a 1-12 months-old newborn published mast cell infiltration of the bone marrow, lymph nodes, spleen, kidneys, and pancreas.
For excellent affected person schooling instruments, discuss with eMedicineHealth's allergic reactions heart. additionally, see eMedicineHealth's affected person education articles allergic reaction and severe hypersensitivity (Anaphylactic Shock).
PreviousNextPathophysiology
Systemic mastocytosis (systemic mast cell disease) is characterized via mast cell infiltration of extracutaneous organs. Mast cells usually infiltrate the bone marrow and as a result impact the peripheral blood and coagulation machine.[15] Mast cells are derived from CD34+/ equipment+ pluripotent hematopoietic cells in the bone marrow.[16] The neoplastic clone of mast cells specific abnormal cell floor markers CD25 and/or CD2. The marrow cellularity ranges from normocellular to markedly hypercellular changes. Erythropoiesis is usually normoblastic with none significant abnormalities. Eosinophilia is a standard bone marrow histology finding (see Workup, Histologic Findings). Hypocellular bone marrow and myelofibrosis can also be seen in late levels of systemic mastocytosis (systemic mast cell disease).
Ho et al evaluated the plasma degree of pro–main normal protein (proMBP), a precursor of major normal protein that's contained in eosinophil cytoplasmic granules, in eosinophilic and power myeloproliferative disorders.[17] They found that the plasma proMBP degree was considerably better in sufferers with systemic mastocytosis (systemic mast cell illness) with eosinophilia, idiopathic eosinophilia, and myeloproliferative problems with eosinophilia than in healthy controls. as well as, the median proMBP level of sufferers with postpolycythemic myeloid metaplasia and those with postthrombocythemic myeloid metaplasia was considerably better than in those with polycythemia vera and crucial thrombocythemia.[17]
Ho et al additionally said that the presence and measurement of splenomegaly used to be correlated with proMBP levels in sure conditions. In sufferers with idiopathic eosinophilia, the presence of splenomegaly was once significantly related to elevated proMBP.[17] In seventy six patients with de novo myelofibrosis, the proMBP stage was once correlated with spleen dimension and the presence of hypercatabolic signs. All of these find ings led the investigators to conclude that "significantly accelerated ranges of proMBP in myelofibrosis patients implies that proMBP may be the most important stromal cytokine in bone marrow fibrosis."[17]
Focal mast cell lesions within the bone marrow are found in roughly 90% of grownup patients with systemic mastocytosis (systemic mast cell illness). a typical mast cell has a spindle-shaped nucleus and effective eosinophilic granules, which can also be visualized at excessive magnification. These cells are prone to return positive findings upon Giemsa staining. Peripheral blood can convey anemia, leukopenia, thrombocytopenia, and lymphopenia. the most common abnormality found in the peripheral blood is anemia. In some patients, eosinophilia, leukocytosis, basophilia, thrombocytosis, and monocytosis may also be observed.
Spleen and lymphoid tissue involvement is a big manifestation of systemic mastocytosis (systemic mast cell illness). Mast cell infiltrates within the spleen can lead to nodular areas that may be perplexed with lymphomas. A biopsy specimen from the spleen can disclose findings much like a myeloproliferative disorder or furry cell leukemia. Histopathology research of the spleen can divulge 2 types of involvement: (1) diffuse infiltration of the red pulp and sinuses and (2) focal infiltration of the white pulp. Lymph node biopsy can express mast cell infiltrates, particularly in the paracortex. Follicles and medullary involvement can also be noticed in some instances.
The immune machine is affected attributable to the in the past talked about pathology. Mast cell merchandise, comparable to interleukin four (IL-four) and interleukin 3 (IL-three), could result in immunoglobulin E (IgE) synthesis and increase T-cell differentiation towards an allergic phenotype. Mast cells also unlock histamine, which ends up in inhibition of interleukin 2 (IL-2).
GI involvement includes microscopic infiltration of the liver, pancreas, and intestines by means of mast cells.[18, 19] belly ache has been attributed to peptic ulcer disease, involvement of the GI tract via mast cells, mediators launched by means of mast cells, and motility problems. GI involvement includes esophageal involvement (eg, esophagitis, stricture, varices), gastric involvement (eg, peptic ulcer illness, mucosal lesions), small gut involvement (eg, dilatated small bowel, malabsorption), colon and rectal involvement (eg, multiple polyposis, diverticulitis), and liver involvement (eg, hepatomegaly and portal hypertension, ascites, sclerosing cholangitis, Budd-Chiari syndrome).
Systemic mastocytosis has many features widespread to myeloproliferative problems and is now included underneath the umbrella of myeloproliferative neoplasm (MPN).[13] Systemic mastocytosis is sort of always associated with the equipment D816V mutation. This acquire of operate kit receptor mutation is detected by using polymerase chain response (PCR) tactics in sixty eight% of bone marrow specimens in sufferers with systemic mastocytosis.[9] further molecular markers being tested embody mutations of JAK2, MPL, and TET2. The affiliation between JAK2 V617F and systemic mastocytosis is susceptible and used to be mentioned in simply four% of patients with systemic mastocytosis (all had related non–mast cell hematological disease).[9] The incidence of TET2 mutations (reportedly as high as 29% in package+ systemic mastocytosis) appears to steer the phenotype without affecting the prognosis.[20]
PreviousNextEpidemiologyFrequencyUnited States
Systemic mastocytosis (systemic mast cell disease) is an extremely uncommon dysfunction; the particular incidence has no longer been said.
global
Epidemiologic information on the incidence of systemic mastocytosis (systemic mast cell illness) are lacking. Some research in great Britain confirmed 2 circumstances per 12 months from a study inhabitants of 300,000.
Mortality/Morbidity
Systemic mastocytosis (systemic mast cell disease) is a progressive neoplastic disorder that has no known healing remedy. Survival in patients with indolent systemic mastocytosis (ISM), with a median survival of 198 months, just isn't significantly totally different from the overall population. then again, median survival with aggressive systemic mastocytosis (ASM) is 41 months and that with SM-AHNMD (associated hematological non mast cell dysfunction) is 24 months. Mast cell leukemia (MCL) has the poorest prognosis with a median survival of 2 months. Leukemic transformation is rare with indolent systemic mastocytosis.[9]
sex
A mild male preponderance in incidence is referred to.[9]
Age
Mastocytosis (mast cell disease) is more common in kids than in adults, and it is frequently transient and self-limited in youngsters when put next with the grownup model. Onset in these younger than 2 years is cited in fifty five% of patients, and, in an extra 10% of patients, the onset is between the a while of two and 15 years.
development of pediatric cutaneous mastocytosis is uncommon, but no longer so in adults, where it regularly progresses to systemic illness.[4]
The median age at prognosis of systemic mastocytosis in adults is fifty five years. sufferers with indolent systemic mastocytosis have been youthful and symptomatic for a longer length of time as compared with patients with aggressive systemic mastocytosis or SM-AHNMD (with other hematological disorders).[9]
PreviousProceed to scientific Presentation , Systemic Mastocytosis

No comments:
Post a Comment
Note: Only a member of this blog may post a comment.